AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2578-8949/020
*Corresponding Author: Luke Jackson, Department of Dermatology, Italy.
Citation: Luke Jackson, Jonathan Noah, Miguel Seth, and Collin Jared , Skin Care Using Heparinoid Creams for Long-Term Treatment with Oxybutynin Transdermal Patches without Skin Irritation in Elderly OAB Patients. J .Dermatology and Dermatitis. Doi: 10.31579/2578-8949/020
Copyright: © 2018 Luke Jackson. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2018 | Accepted: 20 February 2018 | Published: 26 February 2018
Keywords: heparinoids; overactive bladder; skin care; transdermal patch
Background: Overactive bladder is an age-related urologic disease. An oxybutynin transdermal patch is used to treat overactive bladder; however, long-term use is not advised because of potential adverse reactions at the site of application. The present study aimed to investigate the advantages of administering a combination of heparinoid cream and oxybutynin transdermal patch treatment for overactive bladder in elderly patients.
Methods: Eight patients (>65 years of age) with overactive bladder were included. The heparinoid cream was applied topically for 1 week, and skin hydration and transepidermal water loss were quantified before and after application. Thereafter, patients were treated with a combination of an oxybutynin transdermal patch and a heparinoid cream for 12 weeks, and the sites of application were monitored for adverse reactions. Clinical effects of the combinatorial treatment were assessed based on the overactive bladder symptom score.
Results: Application of the heparinoid cream did not decrease transepidermal water loss, but increased skin hydration and improved dryness. Oxybutynin transdermal patch therapy was not interrupted because no skin irritation was observed at the site of application for 12 weeks, and the overactive bladder symptom score decreased significantly (p<0.05).
Conclusions: Combination treatment with an oxybutynin transdermal patch and a heparinoid cream improved treatment outcomes, suggesting that skin hydration with heparinoid cream is a promising treatment method to ensure appropriate use of oxybutynin transdermal patches in elderly patients with overactive bladders.
The incidence of overactive bladder (OAB) has increased in Japan because of rapid aging of the population [1]. As frequent urination, a major symptom of OAB, decreases the quality of life of patients with OAB [2], therapeutic drugs including muscarinic antagonists and β3-adrenoceptor agonists are administered clinically to improve bladder urine retention. Currently, selective muscarinic antagonists are used as first-line drugs to treat OAB [3] and have been developed as an alternative to oral administration of oxybutynin in order to enhance pharmacotherapeutic tolerance.
The oxybutynin transdermal patch is a sustained-release drug formulation containing oxybutynin hydrochloride [4]. Production of N-desethyloxybutynin (DEO), an active metabolite of oxybutynin, is lower with transdermal patches than with oral formulations because oxybutynin is absorbed through the skin, thereby avoiding the hepatic first-pass effect [5]. Anticholinergic effects of DEO increase therapeutic efficacy; however, they also cause side effects including dry mouth and constipation [6]. Use of oxybutynin transdermal patches maintains DEO at low levels during OAB treatment without affecting the activities of daily living [7]. Long-term use of oxybutynin transdermal patches is associated with an increased incidence of skin irritation at the site of application [8]. Therefore, skin conditions of patients with OAB should be evaluated before applying oxybutynin transdermal patches.
The skin of elderly individuals is often dry because of reduced sebum secretion and hydration of the stratum corneum [9,10]. Dry skin is associated with desquamation of the stratum corneum, erythema, and itching [11]. As a transdermal patch should not be applied to the site of application where an adverse reaction has occurred, skin care is important during treatment with transdermal patches. Although moisturizers are commonly used for skin care [12], in particular, a heparinoid cream is expected to decrease skin irritation caused by the transdermal patch to a greater extent because it has high skin hydrating effects [13]. Therefore, use of heparinoid cream would decrease skin irritation caused by oxybutynin transdermal patches and improve treatment adherence. Previously, we reported that treatment with heparinoid cream before applying oxybutynin transdermal patches significantly relieved skin damage occurring after application of oxybutynin transdermal patches [14]. However, the effects of heparinoid cream in OAB treatment with oxybutynin transdermal patches have not been validated clinically.
The present study was carried out to investigate the effects of a combination of heparinoid cream with an oxybutynin transdermal patch in elderly OAB patients.
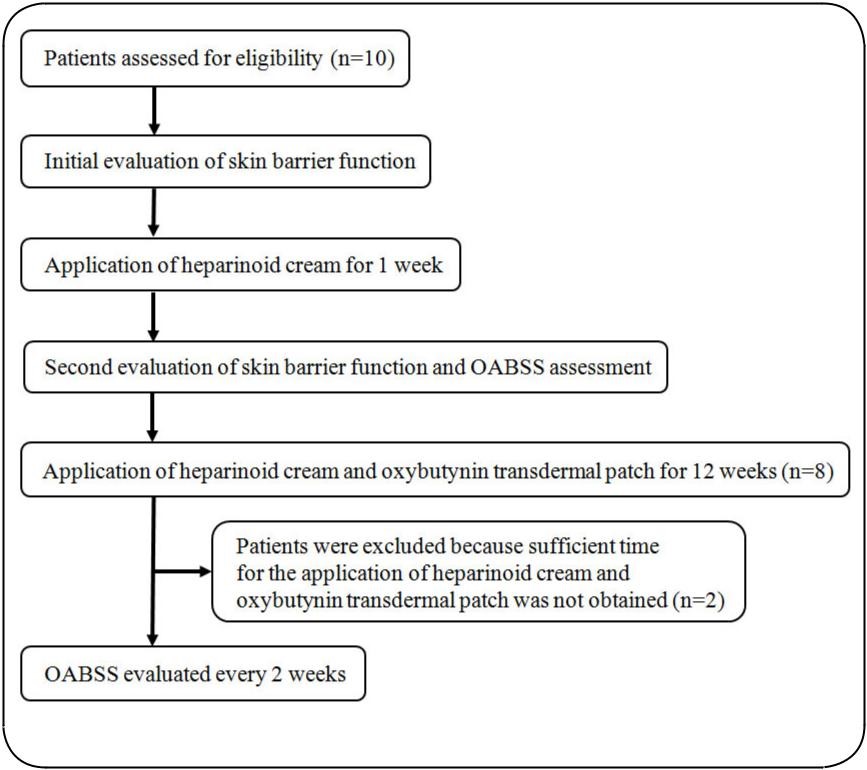
This prospective observational study was performed at the Nagae Prostate Care Clinic according to the procedure depicted in Figure 1. After selecting participants based on the eligibility criteria described in the Participants subsection, heparinoid cream (Hirudoid® soft ointment; Maruho Co., Ltd., Japan) was applied to the skin for 13 weeks. Before application of the heparinoid cream and oxybutynin transdermal patch (NEOXY® TAPE 73.5 mg; Hisamitsu Pharmaceutical Co., Inc., Tokyo, Japan), skin hydration and transepidermal water loss (TEWL) were evaluated at the site of application. An oxybutynin transdermal patch was applied for 12 weeks, and its efficacy and adherence were evaluated every 2 weeks.
Study participants were selected from among OAB patients of both sexes, aged >65 years, who consulted the Nagae Prostate Care Clinic from March to July, 2016. Patients with skin diseases; uroschesis; closed-angle glaucoma; pyloric, duodenal, or intestinal tract blockage; paralytic ileus; gastric or intestinal atony; myasthenia gravis; and those with a history of oxybutynin hydrochloride hypersensitivity were excluded.
Heparinoid cream and oxybutynin transdermal patches were applied based on the schedule depicted in Figure 2. The heparinoid cream (approximately 1 g) was applied twice a day for 13 weeks to the lower abdomen, femoral area, and lower back area of the participants. After 1 week, treatment with oxybutynin patches was initiated. An oxybutynin transdermal patch was applied for 24 h to the right side of the lower abdomen area (Figure 2 {B a}) 1 h after application of the heparinoid cream. From the following day, the oxybutynin transdermal patch was applied consecutively to the skin areas, as illustrated in Figure 2 (B b-f ).
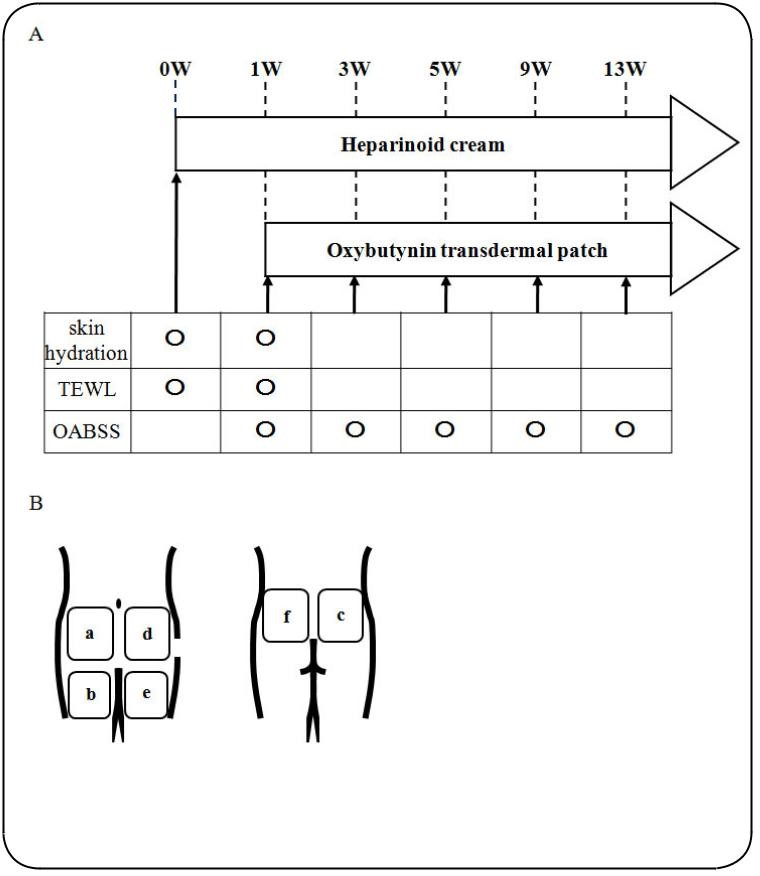
Skin condition in the lower abdomen, femoral area, and lower back of the participants was evaluated before application of the heparinoid cream and oxybutynin transdermal patches, as shown in Figure 2. Skin hydration and TEWL were evaluated using Corneometer CM825 and Tewameter TM300 (Courage and Khazaka Electronic DmbH, Cologne, Germany), respectively, in a room at 45-55% humidity and at 20–25°C.
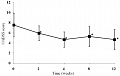
OAB severity was evaluated on the basis of the OABSS, assessed every 2 weeks from the initiation of oxybutynin transdermal patch treatment (week 2). A reduction in OABSS of >3 points during treatment period was considered to indicate effective treatment according to the evaluation method described by Gotoh et al. [15].
All data are presented as the mean±standard deviation (SD) values. Statistical significance of differences between group means was determined using the Mann–Whitney U test. A P-value less than 0.05 indicated statistical significance.
This study was approved by the ethics committee of Suzuka University of Medical Science (approval number: 2016-3-256) and written consent was obtained from all participants in accordance with the tenets of the Declaration of Helsinki.
Effects of heparinoid cream on skin hydration and TEWL
No significant differences were observed in skin hydration at the lower back area after application of the heparinoid cream; however, skin hydration in the lower abdomen and femoral areas improved significantly (Figure 3). No differences were observed in TEWL levels (Figure 4).


No dermatological side effects were observed in any of the patients during treatment with the oxybutynin transdermal patch. The average OABSS decreased from 7.5 points to 4.63 points after 12 weeks of treatment (Figure 5), with 5 of 8 patients (70%) reporting a reduction of >3 points in the OABSS.
In this study, we investigated the effect of heparinoid cream application on the outcomes of treatment with an oxybutynin transdermal patch in elderly patients with OAB. To fulfill our study objective, 10 patients were assessed for eligible skin barrier function. Two patients were excluded because of an insufficient duration of application of the heparinoid cream and oxybutynin transdermal patch. Finally, eight patients (6 males and 2 females) were included in the study.
OAB treatments using oral anticholinergic drugs decrease the quality of life of patients because of anticholinergic side effects such as dry mouth, drowsiness, and coprostasis [16,17]. Oxybutynin transdermal patches have a few associated anticholinergic side effects and are important in treating OAB while maintaining the quality of life of patients. However, effective treatments with oxybutynin transdermal patches are discontinued after 3 months in approximately 64% of cases [18]. Furthermore, Yamaguchi et al. reported that mild reactions occurred at the site of application in 30.3% of elderly patients treated with an oxybutynin transdermal patch [8]. Recently, sustained application of heparinoids has effectively prevented skin irritation at the site of application of transdermal patches [19]. No oxybutynin transdermal patch-associated skin irritation was observed during this study. Our results revealed a reduction in the incidence of adverse reactions at the site of application and higher continuity rates than those reported previously. The OABSS rates four symptoms: daytime urinary frequency, nighttime urinary frequency, urgency, and urgency incontinence; a reduction in the total OABSS reflects effective OAB treatment. In this study, the mean OABSS after 12-week treatment was 4.63 points. As the mean OABSS reported after the oral administration of propiverine hydrochloride and oxybutynin hydrochloride was 4.65 points [20], the therapeutic effects of the combination of the oxybutynin transdermal patch and heparinoid cream explored in this study were considered adequate. These results suggest that application of heparinoid cream effectively prolongs the period of safe use of oxybutynin transdermal patch for OAB treatment without compromising therapeutic effects.
The onset of skin irritation at the site of application of transdermal patches depends on the state of the skin surface [21]. The skin of elderly individuals is easily affected by external stimuli such as cold or dry climate and use of soaps and harsh cleansers because of reduced barrier function and skin hydration caused by aging-related reduction in sebum secretion [22]. Hence, it was speculated that heparinoid cream inhibited skin irritation after application of oxybutynin transdermal patches by moisturizing the dry skin of elderly patients. However, after 1 week of heparinoid cream application, TEWL, which is indicative of skin barrier function, remained unchanged, although skin hydration increased significantly. TEWL was previously reported to decrease after application of a heparinoid-based moisturizer [23]. However, increased TEWL was reported immediately after the application of a moisturizer because of evaporation of water in the formulation [24]. The barrier function of the stratum corneum also reportedly improved after 1 week of application of the heparinoid cream [25]. The dosing time for the eight patients was limited to 1–2 h because the participants in this study were outpatients at Nagae Prostate Care Clinic and a consistent application time was required for the heparinoid cream and oxybutynin transdermal patch for all patients. Hence, the dosing interval of the medications had to be set to 1 h, although TEWL was still quantified accurately. Therefore, high TEWL values observed in this study probably resulted from the evaporation of water from the heparinoid cream, considering that skin hydration function was improved.
Currently, the use of transdermal patches on the skin treated with creams, lotions, or powders is often not feasible owing to decreased skin adhesion. Takai et al. reported that skin adhesiveness of lidocaine tapes was not affected upon application of a heparinoid-based moisturizer [19]. Similarly, in this study, adhesion of oxybutynin transdermal patches was not affected by prior application of the heparinoid cream. Additionally, Björklund et al. reported that skin hydration increased its permeability to metronidazole [26]. Since prior application of the heparinoid cream significantly increased skin hydration in this study, transdermal absorption of oxybutynin hydrochloride may have been altered. Further fundamental animal studies evaluating transdermal absorption of oxybutynin hydrochloride after application of the heparinoid cream are required to adequately assess the proposed use of oxybutynin transdermal patches in combination with heparinoid cream.
Skin care using heparinoid creams has allowed for long-term treatment with oxybutynin transdermal patches without skin irritation in elderly OAB patients. This has also led to fewer side effects and prolonged treatment with stable pharmacological effects. As this technique has circumvented adverse dermatological effects associated with transdermal patches, it has potential applications in general utility for transdermal drug delivery. Drug therapy with transdermal patches has become increasingly important in recent years as the elderly population is increasing. Evaluation of the effects of moisturizers in decreasing skin irritation caused by transdermal patches plays an important role in drug treatment for elderly patients.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.





























































